The Teaching Model
Our training model has been carefully devised by senior doctors with extensive experience in resuscitation and is designed to be an introduction to life-saving skills for everyone – regardless of previous knowledge or experience.
It teaches four simple, yet vital, practical skills emphasising rescuer safety and calling for help early. These skills, when applied in those first minutes following choking or collapse, have been shown to save lives and improve outcomes after sudden cardiac arrest.
There’s no expectation for the children who receive our training to become “First Responders.” Training is offered so that they know what to do if they are in a situation with a collapsed or choking casualty, and can help if they would like to-especially if they are at home on their own and the casualty is a parent or carer.
Our model teaches four skills:

Recognition and Management of a choking child

Recognition and Management of collapsed child – hands-only CPR

Recognition and Management of a collapsed adult – hands-only CPR

Recovery Position
Our sessions teach hands-only CPR (Cardiopulmonary resuscitation) which is simple to learn, easy to remember and most importantly, can help save a life.
To deliver the session, we require the school to provide the following:
The school hall (or a large studio or similar with empty floor space).
At least one DBS checked member of teaching staff to supervise the session directly.
Audio Visual Capabilities to show our skills demonstration video.
Once a school has booked, we will provide the following:




Training Session Materials
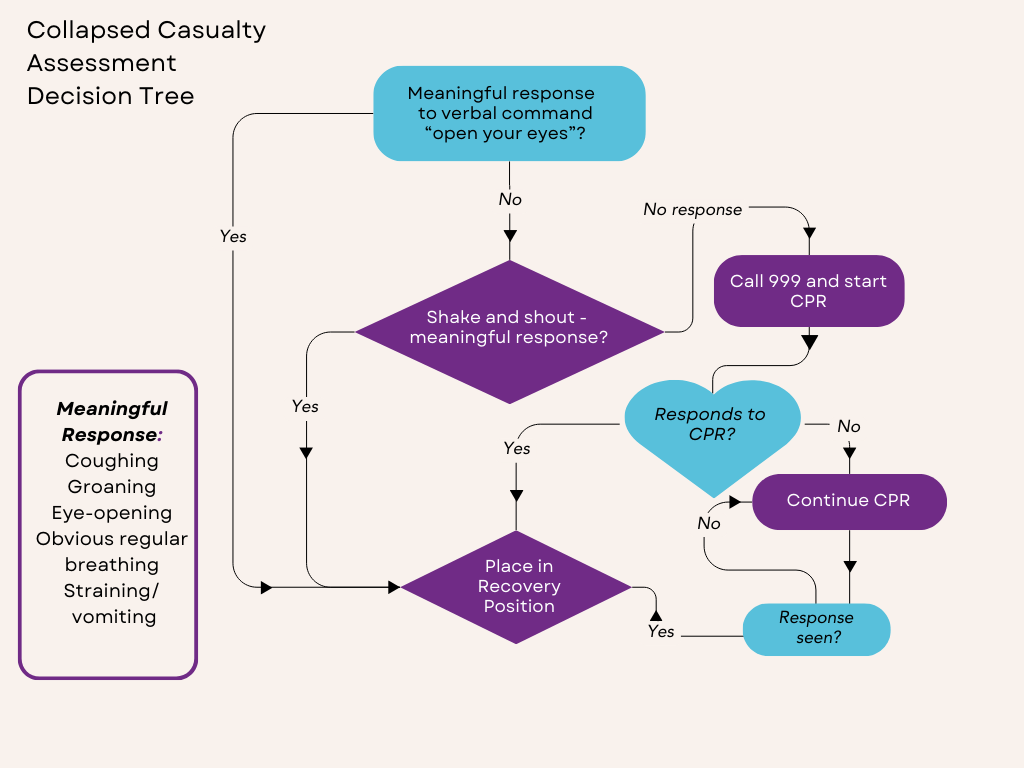
Casualty Assessment and Decision Making
We have kept the casualty assessment very simple, with a “shake-and-shout” action to elicit a meaningful (movement, eye-opening or speech) response and deliberately does not include breathing or pulse checks, This is to avoid:
- mistaking agonal breathing for breathing
- rescuer indecision/inaction because they are unsure of response
A certificate with the skill sequences is made available for the children after the session to help them remember the skills.
Our training is designed to:
- Be simple and memorable. Non-medically trained adults can feel confident teaching it to children.
- Share simple knowledge and skills; so that if the rescuer (adult or child) finds themselves confronted with a collapsed or choking casualty, they know what to do in those first moments.
- Explain and emphasise the need for the rescuer to stay safe and summon help early.
- Have simple casualty assessments so that the rescuer knows what to do next.
- Be in line with current Resuscitation Council guidance, for action by non-medically trained rescuers.
Little LifeSavers training, is designed to be learned by each and every adult member of the population, so they can have these life-saving skills for themselves. Teaching children allows our volunteers to regularly practice these skills and so increase their confidence to use them should they ever need to.
By recruiting adult members of the public to learn this model of “hands-only” CPR, we can help save lives today. By asking those adults to teach school children a few times a year, we empower and equip children; and so save lives tomorrow.

The government added first aid in schools to the curriculum in 2020. Although lesson plans and resources have been provided; no provision to teach basic skills face-to-face has been made to our knowledge. Our Charity began in 2016 before first aid was added to the curriculum, because these skills are so important. Research has shown that many people are still reluctant to perform CPR. https://warwick.ac.uk/newsandevents/pressreleases/nearly_a_third
By reaching out and teaching children four very simple skills we hope to equip and empower them to feel they can step up and provide assistance should they see a child choking or collapse, or an adult collapse.
In time this will create a society where it is the norm to step up and offer assistance – rather than be reluctant to get involved.
Our training is designed to equip and empower them to feel confident in recognising when someone needs assistance, because of choking or collapse. They will be able to quickly assess a casualty whilst staying safe, and take immediate first action and summon help quickly. The training is there to empower them so they can act and not feel helpless.
There is no expectation for them to become first responders or to be summoned to attend to casualties that are not in their immediate vicinity. The training will empower them so that they have some basic skills if they are at an event – for example at home with a sibling. The choice to get involved and offer assistance to a casualty remains entirely theirs.
Rescue Breaths (mouth-to-mouth) should be performed if the rescuer is both trained AND happy to do so. We do not teach rescue breaths for the following reasons:
- They are technically difficult to perform successfully – even by trained medical professionals.
- They interrupt chest compressions.
- Rescuers are often reluctant to perform them – especially on casualties who have vomited.
- Reluctance to perform rescue breaths has been linked to lower incidences of bystander CPR.
- The recommendations for CPR during Covid-19 from the British Heart Foundation and Resus Council UK, are to not perform rescue breaths.
We acknowledge that in paediatric cardiac arrest (especially in younger children), low oxygen levels are the most common reason for the heart to stop. However, hands-only CPR is still a valid and useful technique and increases the chance of survival over not receiving CPR at all.
https://www.bhf.org.uk/how-you-can-help/how-to-save-a-life/how-to-do-cpr/performing-cprduring-covid-19
We teach our child rescuers to perform a brisk “shake-and-shout” assessment to attempt to elicit a response. This removes the need to bring the rescuers face into close contact with the casualty’s face (thus reducing the risk of Covid-19 transmission) and also removes the issue of not being sure of the response.
It can be difficult to tell if a collapsed casualty is breathing at all, breathing normally, or to be able to feel a pulse; especially through clothes and in a noisy environment.
If the child-rescuer does not know if a pulse is present or if the casualty is breathing, they will not
know what to do next. This risks them stopping resuscitation altogether, which, if the casualty needs chest compressions, they will not receive. Their chances of survival then decrease significantly.
Casualties who are not breathing normally and do not have an adequate pulse will need CPR. Our simple assessment gives a clear response – the casualty either speaks, moves, gasps, moans, or they do nothing – meaning the rescuer knows what to do next.
If compressions elicit a response from the casualty we teach the rescuer to stop and to put them into the recovery position and re-check them frequently until help arrives.
Chest Compressions are very stimulating. If a casualty has fainted, they are very likely to regain consciousness at the stimulus of a chest compression and thus respond. This will trigger the rescuer to stop compressions and place the casualty into the recovery position.
There is very little evidence to show injury, or a bad outcome, for a casualty who received compressions they didn’t need. This is in contrast to those who did not receive compressions when they needed them. Resuscitation Councils globally recommend that if a casualty is unresponsive and rescuers are not sure if they are breathing or have a pulse, then they should start hands-only CPR.
https://resus.org.au/faq/will-i-do-harm-if-i-give-chest-compressions-to-someone-with-a-beatingheart/
Current guidance suggests that you should if you can, to reduce the risk of Covid-19 infection.
We take a very practical approach to this advice and suggest that if the casualty has a facemask it can be applied before chest compressions begin. But, unless a cover is immediately to hand, the commencement of CPR must not be delayed by looking for face covering.
We would not recommend covering the face of a casualty who is a young child; and that any face coverings used, must not be a risk to blocking off the casualty’s airway.
We make it clear in the sessions to the children that sometimes resuscitation efforts don’t work and people whose hearts have stopped can still die. It is important to understand that it is not because
the rescuers did anything wrong.
By summoning help and performing chest compressions early, the casualty has been given the very best chance of survival and that is the important thing. It’s just sometimes that the reason for their heart-stopping, or their underlying health being poor, was too severe for them to survive, even with perfect assistance. Support is offered for rescuers such as:
https://www.bhf.org.uk/informationsupport/support/support-if-youve-given-cpr